Amniotomy, or artificial rupture of membranes (AROM), is a procedure in which a healthcare provider manually breaks the amniotic sac to induce or speed up labour. This is done by puncturing the amniotic sac with an amnihook, a long plastic device resembling a crochet needle. The procedure is typically carried out when the cervix is dilated to at least 3 cm, and the fetus is in a vertex presentation with the head well-applied to the cervix. AROM is often used to augment labour in cases of slow progress or to facilitate internal monitoring of the baby. While AROM can shorten the time to delivery, there are potential risks, including increased fetal heart rate abnormalities, cord prolapse, and a higher risk of infection with prolonged ruptured membranes.
| Characteristics | Values |
|---|---|
| Procedure | Amniotomy, or artificial rupture of membranes (AROM) |
| Purpose | To induce or expedite labour, or to place internal monitors |
| Timing | Performed at the bedside in the labour and delivery suite |
| Indications | Internal fetal or uterine monitoring is needed, induction of labour, augmentation of labour |
| Contraindications | Known or suspected vasa previa, contraindications to vaginal delivery, unengaged presenting part |
| Effectiveness | The American College of Obstetricians and Gynecologists (ACOG) recommends waiting longer to perform AROM in low-risk pregnancies |
| Benefits | May speed up labour, stronger and more regular contractions, allows assessment of amniotic fluid, enables internal monitoring |
| Risks | Quick increase in contraction intensity, umbilical cord compression, difficulty for baby to rotate, increased risk of infection, umbilical cord prolapse, severe blood loss to baby |
Explore related products






What You'll Learn
![]()
Amniotomy is a mechanical method for induction of labour
Amniotomy, or artificial rupture of membranes (AROM), is a mechanical method for induction of labour. It involves rupturing the amniotic sac to release amniotic fluid and is usually performed to induce or expedite labour or to place internal monitors. The procedure is typically carried out at the bedside in the labour and delivery suite.
Amniotomy is indicated when internal fetal or uterine monitoring is needed, for induction of labour, and for augmentation of labour. It may be contraindicated in cases of known or suspected vasa previa, any contraindications to vaginal delivery, or an unengaged presenting part.
The procedure is generally considered safe and can be performed when the cervix is partially dilated and effaced, with the fetus in a vertex presentation and the head well-applied to the cervix to avoid umbilical cord prolapse. Fetal monitoring is used during the procedure to evaluate the colour of the amniotic fluid and detect for the presence of meconium staining, which may indicate fetal distress.
The benefits of amniotomy include a potential shortening of labour, stronger and more regular contractions, and the ability to place internal monitors if needed. However, there are also risks associated with the procedure, such as a quick increase in the intensity of contractions, umbilical cord compression, difficulty for the baby to rotate into a better position, an increased risk of infection, and the possibility of the umbilical cord prolapsing, which is a medical emergency.
While some studies suggest that amniotomy is an effective method for induction of labour, the benefits and effectiveness of the procedure are still debated. The American College of Obstetricians and Gynecologists (ACOG) recommends that labour and delivery teams wait longer to perform amniotomy in low-risk pregnancies where mother and baby are progressing normally.
The Magic of Pax Aroma: Enhancing Your Space
You may want to see also
Explore related products






![]()
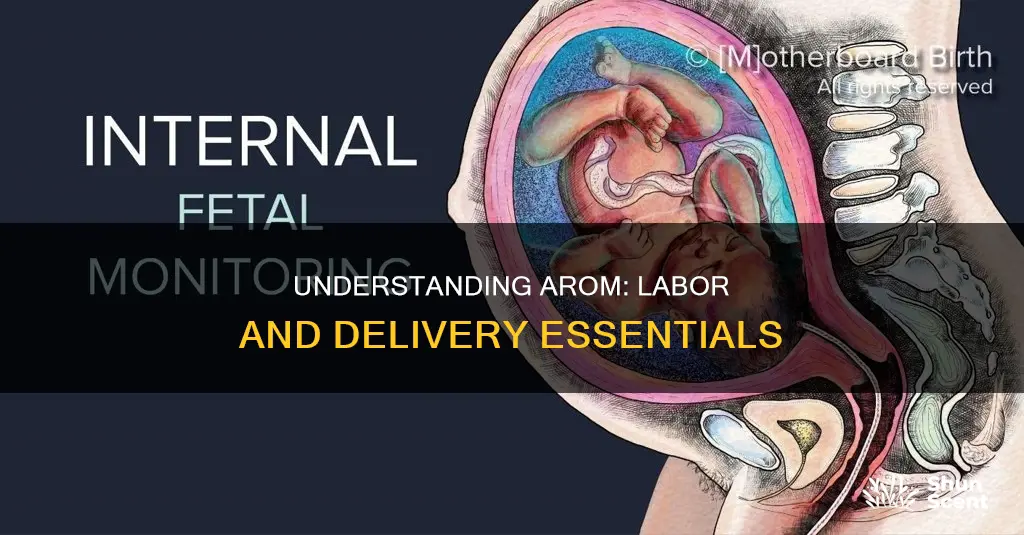
AROM is performed when the cervix is partially dilated
Amniotomy, or artificial rupture of membranes (AROM), is a procedure used to induce or augment labour by rupturing the amniotic sac. AROM is performed when the cervix is partially dilated and effaced, and with the fetus in a vertex presentation. The procedure is typically carried out using an amnihook, a long plastic device that creates a small opening in the amniotic sac.
AROM is generally considered safe if the presenting part is well-applied to the cervix, and is often accompanied by fetal monitoring to evaluate the colour of the amniotic fluid for meconium staining, a possible indication of fetal distress. The procedure is also used to inspect the nature of the amniotic fluid, especially in high-risk cases or if the fetal heart rate pattern is abnormal.
The appropriate timing of AROM is debated, as earlier rupture of membranes may lead to a longer exposure to ruptured membranes during labour, potentially increasing the risk of infection. However, performing AROM at 4 cm dilation may shorten the time to delivery without increasing the risk of infection. The combination of AROM and intravenous oxytocin is the most effective induction method for a favourable cervix.
AROM is often used to augment an abnormal first stage of labour, particularly in nulliparous women, and has been shown to reduce the median length of time to progress to complete cervical dilation and reduce the rate of labour dystocia. It can also be used to evaluate the amniotic fluid for meconium, facilitate the application of internal monitoring devices, and reduce the time in labour.
While AROM can be beneficial, there are potential risks and adverse effects associated with the procedure. These include an increased risk of umbilical cord prolapse, especially if the fetal head is ballotable, as well as an increased risk of maternal or fetal infection, fetal laceration, scalp infection, cephalohematoma, and malalignment of fetal cranial bones. A Cochrane review found that AROM was associated with an increased caesarean section rate and a near-statistical increase in the rate of caesarean delivery.
The Bible and Aromas: A Fragrant Journey Through Scripture
You may want to see also
Explore related products






![]()
The procedure is carried out by an Amnihook
Amniotomy, or artificial rupture of membranes (AROM), is a procedure to break the amniotic sac and induce labour contractions. The amniotic sac is a fluid-filled sac that surrounds and protects the foetus during pregnancy.
The Amnihook is considered safe and secure for rupturing the amniotic membranes before and during labour. The procedure is generally well-tolerated, with most people not feeling anything, especially if they are already in labour or have had an epidural.
Wine Aroma: Unlocking Secrets in Every Bottle
You may want to see also
Explore related products






![]()
AROM can be used to speed up labour or help induce it
Amniotomy, or artificial rupture of membranes (AROM), is a procedure that can be used to speed up labour or help induce it. AROM involves rupturing the amniotic sac to induce labour contractions. The amniotic sac is a fluid-filled sac that surrounds the foetus during pregnancy, providing protection, cushioning the fetus, and softening its movements while in the uterus.
AROM is performed when the cervix is partially dilated and effaced, and with the fetus in a vertex presentation with the head well applied to the cervix. This helps to avoid prolapse of the umbilical cord or other presenting parts. The procedure is typically carried out using an amnihook, a long plastic device resembling a large crochet needle, which is inserted into the vagina to puncture a hole in the amniotic sac.
The effectiveness of AROM is often debated, and some studies suggest that it may not be effective in advancing labour in low-risk pregnancies. However, it is believed that AROM can help speed up labour by removing the fluid cushion between the baby's head and the cervix, allowing more pressure to be placed on the cervix, resulting in faster dilation. Additionally, the release of amniotic fluid may encourage a rise in natural oxytocin levels, bringing on stronger and more frequent contractions.
AROM can also be used to facilitate internal monitoring of the baby and to examine the amniotic fluid for meconium levels, which can affect the baby's health and determine the type of medical support required at delivery.
Aroma Taste Inhibitors: How Do They Work?
You may want to see also
Explore related products






![]()
AROM can be used for internal monitoring
AROM, or Artificial Rupture of Membranes, is a procedure in which a healthcare provider breaks the amniotic sac to help induce or speed up labour. The procedure is usually carried out by an obstetrician or a midwife, and involves the use of a long plastic device called an amnihook, which looks like a crochet needle. The amnihook is inserted into the vagina and used to puncture the amniotic sac, leading to a release of amniotic fluid.
Internal monitoring is one of the reasons why AROM may be performed. It can be difficult to track the baby's heart rate using external monitors, so an electrode may be attached to the baby's head through the vagina and cervix. This type of monitoring allows the baby's heartbeat to be monitored continuously, regardless of the position of the mother. Internal monitoring also allows for the intensity of the contractions to be monitored, not just their timing and duration.
AROM is a common procedure that has been performed for hundreds of years. However, the benefits and effectiveness of AROM are debated, and there is conflicting evidence about whether it truly speeds up labour. While some studies show that AROM is an effective method of induction, others suggest that it does not accomplish this outcome.
There are several benefits and risks associated with AROM. On the one hand, it may result in shorter labour, stronger and more regular contractions, and the ability to assess the colour and odour of the amniotic fluid. On the other hand, there is a risk of a quick increase in contraction intensity, compression of the umbilical cord, difficulty for the baby to rotate into a better position, and an increased risk of infection.
The Intriguing Implication of 'Aroma': Scent's True Meaning
You may want to see also
Frequently asked questions
AROM stands for Artificial Rupture of Membranes. It is a procedure in which a practitioner manually breaks the amniotic sac to speed up labor and contractions.
AROM is performed to speed up labor or to help induce labor. It is also used when internal fetal or uterine monitoring is needed.
AROM is performed by a healthcare provider, either an obstetrician or a midwife. The procedure is typically carried out by inserting an amnihook, a long plastic device that looks like a crochet needle, into the vagina to puncture the amniotic sac.
Some benefits of AROM include a shorter labor and stronger, more regular contractions. AROM also allows providers to assess the color and odor of the amniotic fluid. Risks of AROM include a quick increase in the intensity of contractions, possible umbilical cord compression, and an increased risk of infection if the amniotic sac is ruptured for too long.